Introduction: Malignant Rhabdoid tumors (MRT) are among the most aggressive and lethal forms of infant and child cancer (1). These tumors are characterized by an unusual combination of mixed cellular elements similar to but not typical of teratomas and can originate at any anatomic location. When MRTs are present in the brain, they are called atypical teratoid/rhabdoid tumors (AT/RT), which accounts for 1-2% of central nervous system tumors in children (2). Genetically, MRTs typically demonstrate abnormalities in the SMARCB1 gene located on chromosome 22, which influences the SWI/SNF chromatin remodeling complex that is involved in regulating cell cycle, growth, and differentiation (2). Because of the influence on different cell cycle processes, SMARCB1 is understood to be a tumor suppressor gene. Although most mutations in SMARCB1 primarily occur de novo, familial cases have been reported and if inherited leads to a condition called rhabdoid tumor predisposition syndrome (RTPS). Genetic testing of genes associated with RTPS may confirm diagnosis and help guide treatment options. Herein, we will cover how VS-CNV (VarSeq’s CNV Caller) identifies a structural variation associated with rhabdoid tumors and how VSClinical identified possible treatment options for this rare disease.
Case Study: A four-year-old presented symptoms of headache, nausea and vomiting without fever. The child also displayed unusual eye movements and problems walking. Magnetic resonance imaging was requested, which identified a small tumor in the brain. A stereotactic needle biopsy was performed and using microscopy it was diagnosed as atypical teratoid/rhabdoid tumors (AT/RT). To validate these findings blood samples were taken for genetic testing and VCF and BAM files were created.
VS-CNV: The VCF and BAM files were imported into VarSeq and were evaluated for pathogenic single nucleotide variants (SNVs) according to the ACMG and AMP guidelines. Using this approach did not result in a conclusive pathogenic SNVs associated with rhabdoid tumors. Using the same platform, the BAM file was then used to identify the presence or absence of structural variations or copy number mutations using protocol outlined in this webcast and tutorial. The results showed a duplication event in exon 6 of the SMARCB1 gene that was not associated with any quality flags and had a p-value below 0.001, Figure 1. This event was then added to VSClinical to be evaluated using the AMP guidelines.
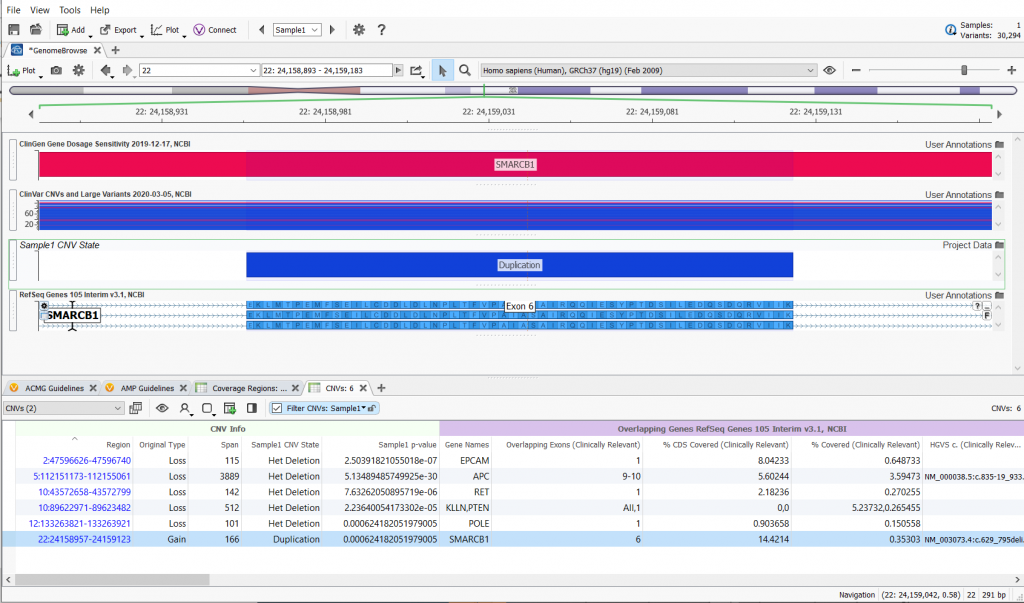
Figure 1: An amplification of exon 6 in the SMARCB1 gene was identified using the existing coverage stored in the BAM file.
VSClinical AMP Workflow: In the AMP guidelines interface the patient and sample information was entered and Central Nervous System/Brain was selected for the Tissue with Rhabdoid Meningioma (RHM) selected as the Tumor Type, Figure 2. After the SMARCB1 Exon 6 Amplification was added to the Mutation Profile, the CNV was then evaluated as a biomarker in the Biomarker Tab.
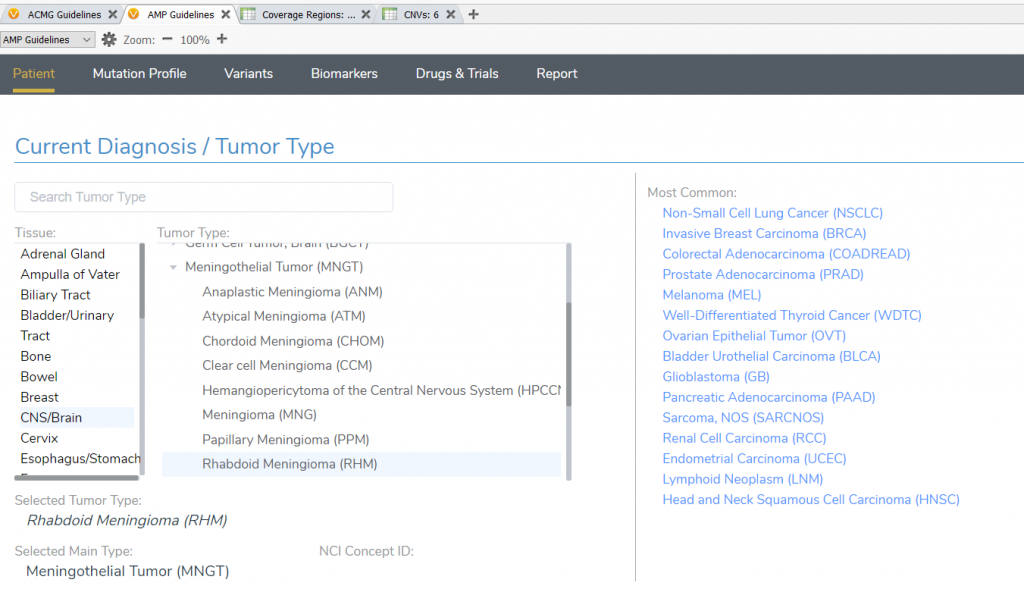
Figure 2: In the VSClinical AMP Workflow interface the Selected Tumor Type was set to Rhabdoid Meningioma.
In the Biomarker tab a detailed gene summary was provided by the annotation database, Genetic Home Reference, as well as the other somatic annotation databases, Figure 3. In summary, SMARCB1 creates a subunit of the SWI/SNF protein complexes, which regulate gene activity by chromatin remodeling. Other processes include repairing damaged DNA, copying DNA, and controlling growth, division, and maturation of cells. Through these processes, the SMARCB1 protein and other SWI/SNF subunits are thought to act as tumor suppressors.
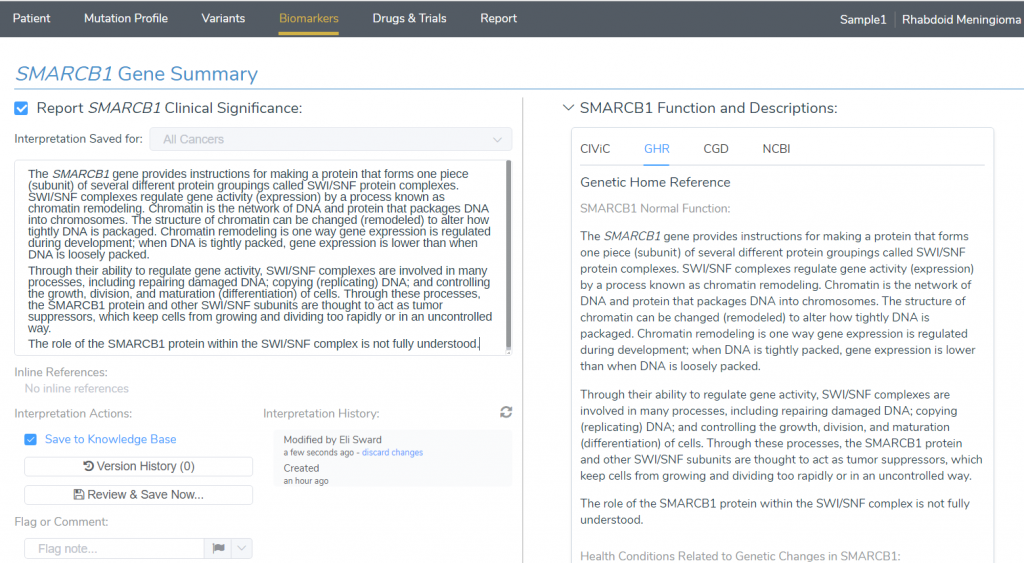
Figure 3: Gene Summary Provided by Genetic Home Reference.
Looking at the SMARCB1 Alteration and Frequency Outcomes in COSMIC, Figure 4, it is evident that alterations in this gene primarily occur in the central nervous system (CNS)/Brain but also in many other anatomical sites.

Figure 4: COSMIC displaying the tissue locations and occurrence of mutation alterations in the SMARCB1 gene.
Clinical Evidence: The Clinical Evidence interface was then used to identify FDA approved drugs or clinical trials. The table contains an integration of relevant clinical sources, specifically DrugBank, PMKB and CIViC and are sorted by the strength of their clinical assertions. Filtering results that were Gene and Tissue Specific resulted in 5 records, Figure 5. The first result is a Clinical Trial with two FDA approved drugs: ALRN-6924 and Cytarabine. By selecting this first option, a detailed description is provided, which can be included in the clinical report. In summary, this is a Phase I clinical trial to test the safety of an investigation intervention and also tries to define the appropriate dose to use for further studies. ALRN-6924 is a drug that blocks certain proteins in tumors cells called MDM2 and MDMX, which may cause tumors to die. The purpose of this study is to find the best dose of ALRN-6924 when used in children and to determine effectiveness against types of cancer seen in children. Since this is a Clinical Trial, the Drugs and Trials interface was then used to identify nearby locations.
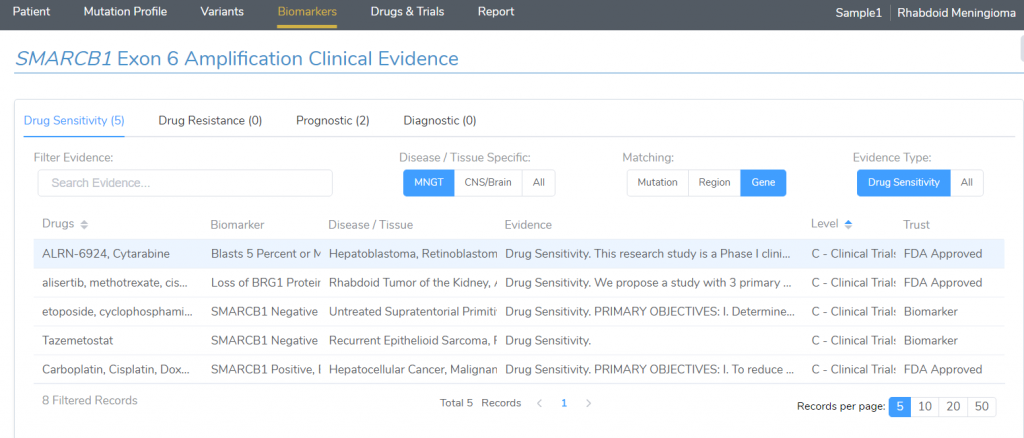
Figure 5: The Clinical Evidence interface identified 5 results for FDA approved drugs or Clinical Trials for matching SMARCB1 gene alterations associated with Rabdoid Meningioma.
Drugs and Trials: This interface allows users to determine the location of clinical trials, if they are recruiting, and if the patient is eligible based on inclusion and exclusion criteria. This clinical trial was found to be active in four different locations with San Francisco being one of them. The eligibility of the trial included being age 1 to 21 and having the biomarker of a SMARCB1 Gene Mutation associated with Rhabdoid Tumor. With our new reporting template, this clinical trial information and biomarker summary can now be included in the clinical report and rendered in an automated fashion, Figure 7.
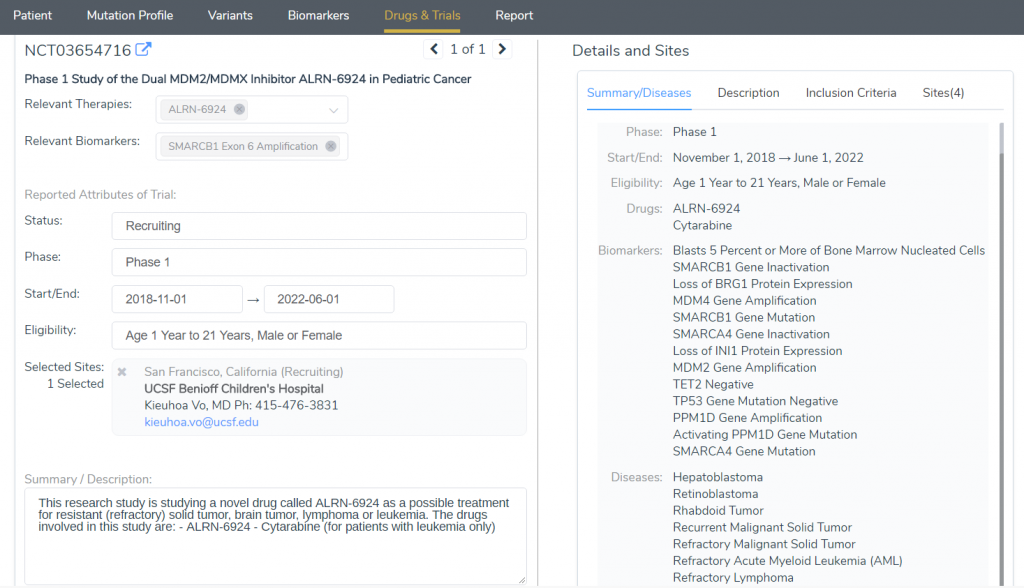
Figure 6: The Drugs and Trials tab identified 4 Clinical Trials that were recruiting for Rhabdoid tumors and SMARCB1 gene alterations.
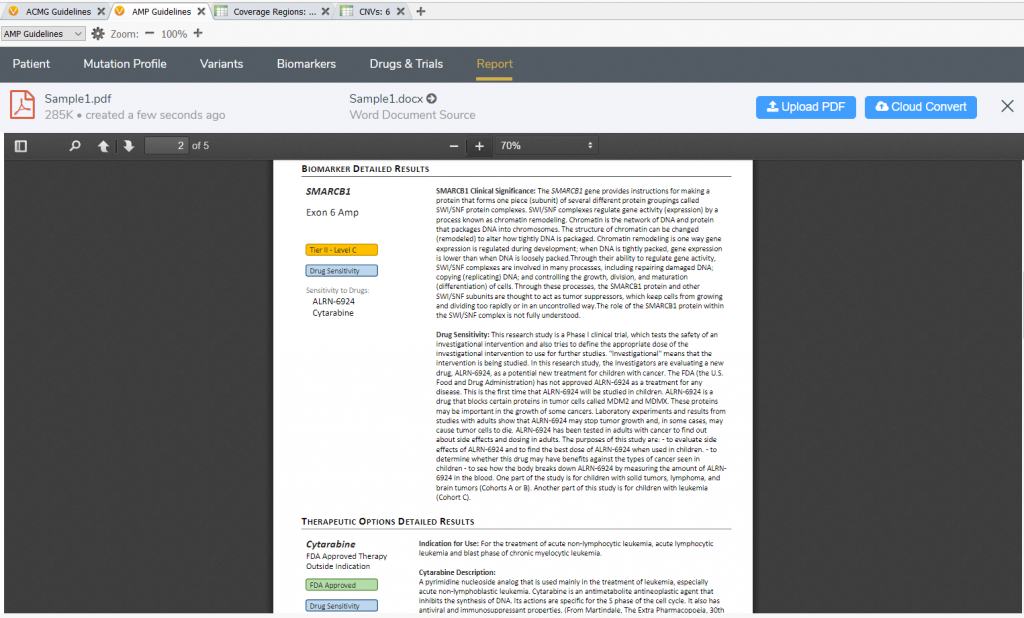
Figure 7: Clinical reporting in VSClinical will automatically pull in all information for the evaluated biomarker, which can be rendered in a word document or PDF format.
Conclusion: Using the VSCNV platform, an amplification of exon 6 was observed in the SMARCB1 gene, which likely was leading to a frameshift mutation whereby the exon could be variably spliced into the mRNA transcript. As the SMARCB1 is a tumor suppressor gene, this alteration was the likely biomarker associated with the rhabdoid tumors identified in the brain of the patient. Using the VSClinical AMP interface, a biomarker interpretation was created and a clinical trial was identified that could be recommended to the patient. Finally, a clinical report was generated using the same platform, which could then be provided to the clinician and patient.
Final notes: I hope this was a resourceful blog in showing users the capabilities of VarSeq, VS-CNV and VSClinical’s AMP Guideline interface. The nice thing about these features is that they are all incorporated in one platform, which can save diagnostic and clinical labs time, money, and resources. If this is something of interest to you, I would highly recommend evaluating our software and testing it with your own data. Here is the link with further details. Lastly, if you have any questions about this blog or regarding our products, please don’t hesitate to comment below or reach out to [email protected].
Thanks for reading! If you liked this blog, check out our other blog WT1 Mutations: Side-by-Side Germline and Somatic Variant Evaluation in VSClinical
Work’s Cited:
- Heck JE, Lombardi CA, Cockburn M, Meyers TJ, Wilhelm M, Ritz B. Epidemiology of rhabdoid tumors of early childhood. Pediatric Bloob Cancer, 2013;60:77-81.
- Sredni SI, Tomita TA. Rhaboid Tumor Predisposition Syndrome. Pediatric and Developmental Pathology, 2015; 18:49-58.



