
Discover powerful WES prenatal workflow examples showcasing the detection of Duchenne Muscular Dystrophy, Gaucher Disease, and Fabry Disease through advanced genetic screening techniques.
Our recent Prenatal Genetic Screening with VarSeq webcast focused on using whole exome analysis for prenatal genetic screening. This webcast was a hit with our customers, who asked for more information on different filtering chains to identify specific genetic conditions. Here, we bring you further examples of prenatal workflows. This blog will show you three of our most in-demand workflow examples: an exonic DMD deletion related to muscular dystrophy, a GBA mutation related to Gaucher disease, and an X-linked variant related to Fabry diseases. First, let’s explore a prenatal screen for a DMD deletion related to Duchenne muscular dystrophy.
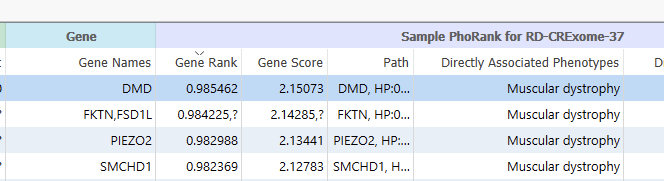
This example is of a WES sample from a proband with a family history of muscular dystrophy. This sample was run in a large batch of samples. For our sample of interest, the phenotype of muscular dystrophy is from a very specific search term. To look for CNVs that are associated with this phenotype, we can use PhoRank to look for CNVs in genes known to be associated with muscular dystrophy (Figure 1). CNV analysis is central to identifying exonic deletions like the DMD variant explored here. PhoRank in itself is an integral part of the filter chain (Figure 2), but as you can see from this screenshot below, there are many CNVs called in this WES sample that could be associated with our phenotype. The goal is to narrow the search to just high-quality CNVs.
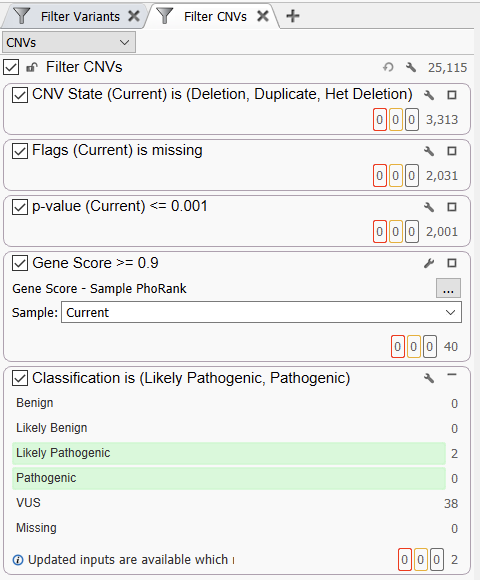
Here we can take a look at a relatively simple CNV filter chain (Figure 2). We first filter on CNV State for variants that are deletions, duplications, or heterozygous deletions. Next, we filter for the lack of quality control flags, then low P-value. After that, we bring in our Sample Phorank search, setting a stringent threshold of 0.9 for an association. Last, we run the ACMG CNV classifier to determine which of the remaining CNVs has a pathogenic score — a key step in variant classification under ACMG/AMP guidelines. Although we saw that there were many CNVs potentially involved with our phenotype (Figure 1), only two of them were high quality.
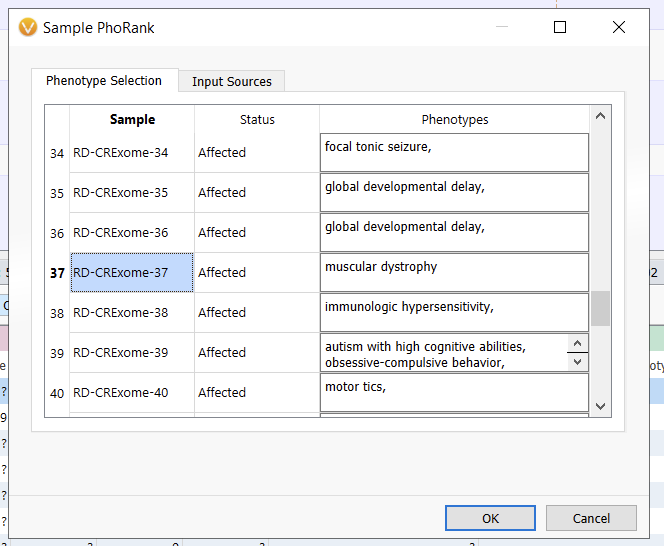
Here we should note that the PhoRank Sample is set to ‘Current.’ As this sample was in a batch of 60 WES samples, each had its own phenotypes to be searched. It is possible to bring these phenotypes in with a text manifest so we can search for specific associations in each of the samples (Figure 3). Through this method, we can efficiently screen a multitude of patient-specific phenotypes while not having to generate multiple workflows.
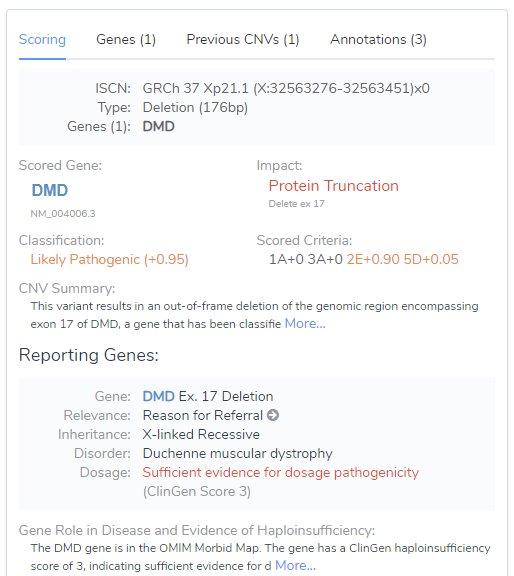
Now that we have isolated our DMD variant, we can go into VSClinical for the review and ultimate report rendering (Figure 4). Below, we can see the details for this particular deletion, which spans 176 bp in length. The scoring box indicates that the impact of the CNV would be a protein truncation and how the classification is Likely Pathogenic based on the scored criteria 2E and 5D. We also see that the disorder has been correctly associated with Duchenne muscular dystrophy and that there is sufficient evidence for dosage pathogenicity. Now that the criteria have been scored and the classification determined, this information can be rendered into a final clinical report to be handed to the clinician.
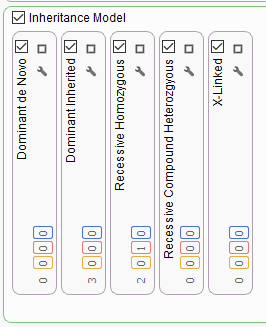
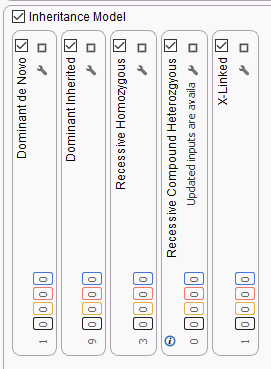
Next, we are going to take a look at a trio workflow that isolated an autosomal recessive variant in the proband. Here, we see our inheritance model, used in many of our trio workflows (Figure 5). Right off the bat, I can see that there are three variants coming through the Dominant Inherited filter and two coming through the Recessive Homozygous filter.
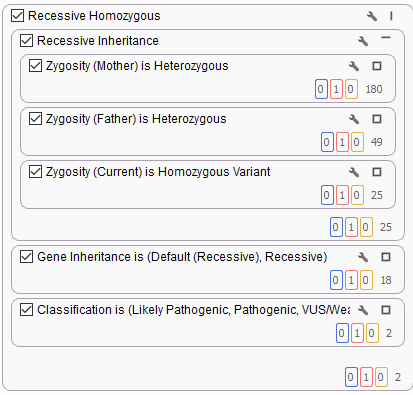
Taking a closer look at the Recessive Homozygous filter container, we can see the first levels look for a heterozygous variant in the mother, and father, but a homozygous variant in the proband (Figure 6). The Gene Inheritance filter brings in variants that are recessive. Finally, the ACMG sample classifier brings in the variants that are Likely Pathogenic, Pathogenic, and VUS/Weak Pathogenic. Overall, two variants make it through this filter chain.
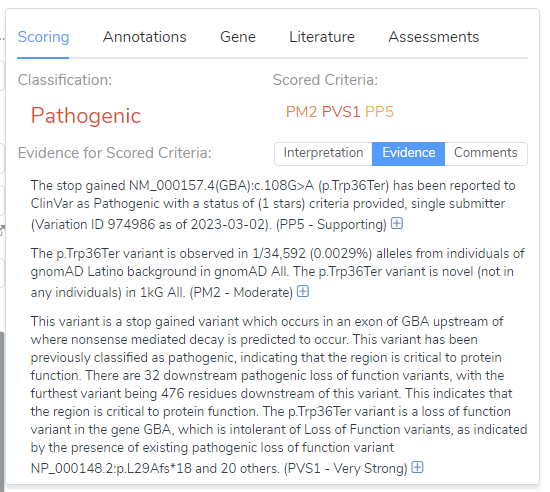
This next view is from inside VSClinical, showing the evidence for scored criteria for our GBA variant (Figure 7). There is a ClinVar submission reporting this variant as pathogenic, bringing us a PP5 criteria. Next, we have a very low allele frequency observed in gnomAD, while it is not observed in 1kG Phase 3. Together, this results in a PM2 criteria. Last, this variant results in a stop gained, therefore rendering a PVS1- Very Strong criteria. Together, this results in a pathogenic variant.
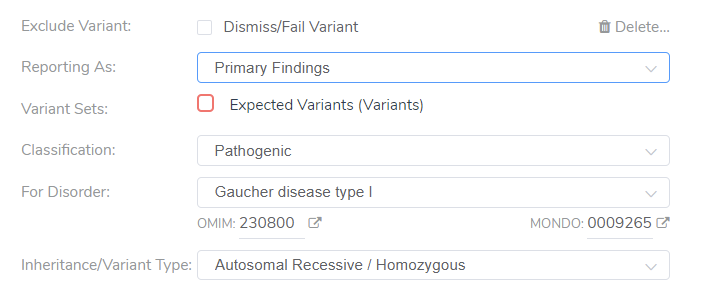
Finally, we have the Reporting section from inside VSClinical (Figure 8). The variant is being reported as a Primary Finding with the Pathogenic classification. The listed disorder is correctly identified as Gaucher disease type I, and the inheritance as autosomal recessive and homozygous. Now that the variant is classified as a Primary Finding, this information can be rendered into a final report to be given to the clinician.
Last, we have an example of an X-linked variant, specifically one in the gene GLA, which is linked to Fabry disease. For this WES trio analysis, the proband is seen to carry one X-linked variant (Figure 9).
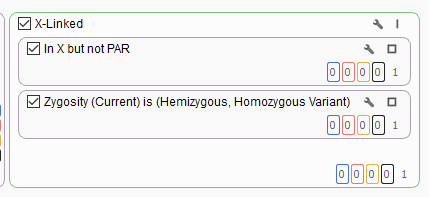
Taking a closer look at the X- linked filter container, we can see that the first container designates a position (Figure 10). This would mean the variant exits in the X chromosome but not in the pseudoautosomal region. Next, we filter on zygosity to look for hemizygous or homozygous variants.
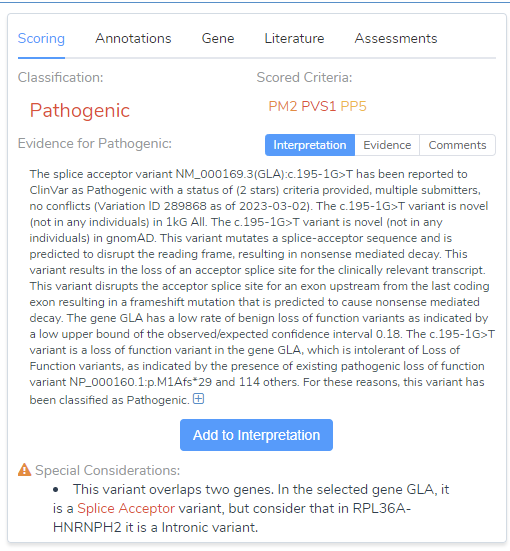
After isolating our variant of interest, we can bring it into VSClinical for analysis. This variant has a PM2 criteria, a PVS1 criteria, and a PP5 criteria (Figure 11). We are also warned that the variant overlaps two genes, the GLA of interest for Fabry disease and RPL36A-HNRNPH2. After consideration, we are in the MANE Select Transcript, and the GLA transcript is in a coding region while the other transcript would be in an intronic region. Therefore, the criteria analysis is sound.
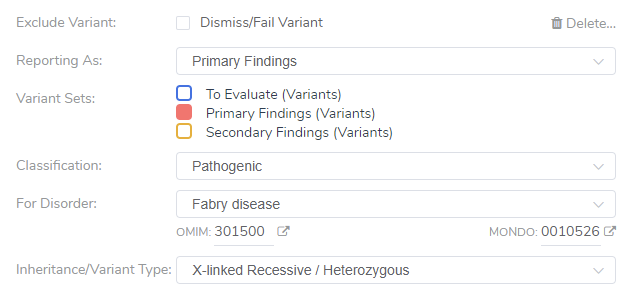
Last, we will report this variant as a Primary Finding with a Pathogenic classification (Figure 12). In addition, Fabry disease has been correctly identified, along with this variant existing as X-linked Recessive.
Now that the pathogenic variant has been identified and classified, the clinician can quickly render this into a final report with VSReports. That report can then be turned around the expectant family.
Thank you for joining us as we go through several more examples of workflows that can be used in the prenatal analysis space. We hope this was helpful, and please reach out to [email protected] if you have further questions or would like assistance customizing your workflows for the prenatal NGS space.




I enjoy what you guys are up too. This kind of clever work and
coverage! Keep up the fantastic works guys!